The Single Strategy To Use For Physiotherapy & Ehlers-Danlos Syndrome / Joint - EDHS.info
from web site
Some Known Incorrect Statements About Shoulder dislocation, instability and hypermobility - Evidence
Hypermobility and hypermobility syndrome prevail conditions with universal interest. However, in spite of significant advances in our understanding of the discussion and ramifications of lax tissues there is still much to discover the very best method to manage the signs. Find More Details On This Page discusses our current knowledge on the management of joint problems associated with hypermobility syndrome.
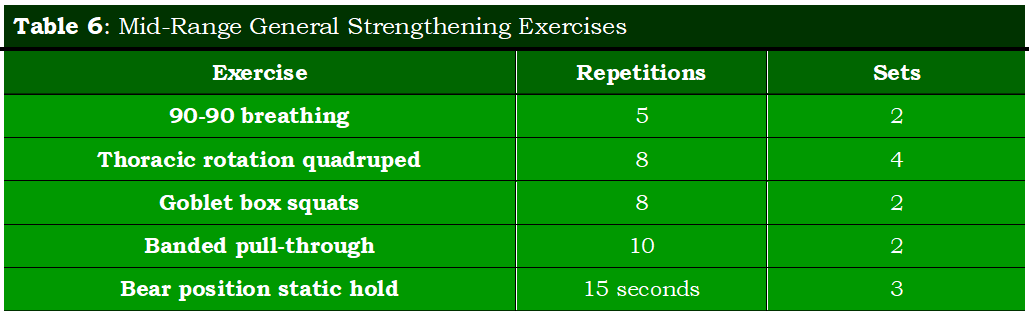

Research has recognized that posture, proprioception, strength and motor control are essential parts in achieving this goal along with education, physical activity and fitness. It is not yet understood what form the optimal physical rehabilitation programme should take, but the parts talked about here are based upon sound clinical principles which it is hoped will further understanding, promote interest and promote further research study.
The hypermobility syndrome(HMS) was very first explained in 1967 by Kirk et al as the occurrence of musculoskeletal symptoms in hypermobile healthy individuals. Meanwhile, other names are provided to HMS, such as joint hypermobility syndrome and benign hypermobility joint syndrome. HMS is a dominant acquired connective tissue condition explained as "generalized articular hypermobility, with or without subluxation or dislocation.
Hypermobility syndrome is different from localized joint hypermobility and other disorders that have generalized joint hypermobility, such as Ehlers-Danlos Syndrome, Rheumatoid Arthritis, Systemic Lupus Erythematosus, and Marfan Syndrome. HMS may take place also in chromosomal and congenital diseases such as Down syndrome and in metabolic disorders such as homocystinuria and hyperlysinemia.

See This Report on REHAB MANAGEMENT OF JOINT HYPERMOBILITY
Clinically Relevant Anatomy [edit modify source] The pathophysiology in Hypermobility Syndrome is not yet completely understood, it appears to be a systemic collagen problem. The problem in collagen ratios is related with joint hypermobility and laxity of other tissues. The ratio of collagen (type I, II and III) is decreased in the skin.
HMS also impacts the joint position sense. Joint hypermobility occurs frequently in kids and lowers with age. Joint mobility is greatest at birth, there is a decline in children around 9 to twelve years old. In adolescent girls, there is a peak at the age of fifteen years, after this age the joint movement reduces, as well in kids as in girls.
